고위험신생아 부모의 퇴원 준비 측정도구: 체계적 문헌고찰
Discharge Readiness Scale for Parents of High-Risk Infants: A Systematic Review
Article information

Trans Abstract
Purpose
Discharge readiness for parents of high-risk infants is an important predictor of successful transitions from hospital to home, however its assessments criteria require further refining in Korea. The purpose of this study is to provide a comprehensive overview of the measures available for assessing the discharge readiness for parents of high-risk infant and to evaluate the measurement properties of each instrument.
Methods
A literature search for discharge readiness for parents of high-risk infants was performed using 8 electronic databases (MEDLINE, Embase, CINAHL, PsycINFO, Web of Science, KoreaMED, RISS, KISS), using preferred reporting items as per the systematic reviews guidelines. For the quality evaluations of the articles, the COSMIN checklist including content validity, internal structure, and the remaining measurement properties was used.
Results
Among the 23 studies selected, 8 studies were excluded due to lack of information on their instrument's measurement properties while remaining 15 studies were evaluated for the quality of measurement attributes. Overall information on the properties of the instruments was lacking in all studies.
Conclusion
None of the instruments evaluated all the relevant measurement properties. The results of this review suggest that it is necessary to develop a discharge readiness instrument that considers the necessary and relevant characteri stics required for successful hospital to home transition for parents of high-risk infants.
서 론
1. 연구의 필요성
지난 20년 동안 우리나라의 합계 출산율은 급격한 감소로 매우 낮은 수준인데 반해, 미숙아 혹은 저체중 출생아의 출산은 계속해서 증가하고 있다(Korea Statistical Information Service, 2021). 또한 신생아치료기술과 간호의 발전으로 미숙아를 포함한 고위험신생아의 생존율은 지속적으로 향상되고 있다(Blencowe et al., 2012). 치료적 개입을 통한 생존율 향상으로 고위험신생아는 퇴원 시점에도 잠재적 건강문제를 가지는 경우가 많다(Kim et al., 2015). 고위험신생아의 신생아집중치료실 퇴원은 지금껏 병원에서 이루어지던 자녀의 간호를 부모가 가정에서 전적으로 맡는 것을 의미한다(Spear et al., 2002).
퇴원 준비는 환자가 급성 치료 시설(병원)을 떠날 수 있는 능력을 평가하는 다차원적 개념이다(Weiss et al., 2008). 즉, 신체적 안정성과 가정에서 증상을 관리할 수 있는 능력, 퇴원 후 대처를 위한 적절한 지원, 퇴원 후 관리를 할 수 있는 심리적 능력, 일반적 문제에 대응하기 위한 적절한 정보와 지식을 포함하는 과정이다(Galvin et al., 2017). 미국소아과학회(American Academy of Pediatrics)에서 발표한 고위험신생아 퇴원 지침에 따르면 퇴원 시기를 결정하기 위해서는 고위험신생아의 퇴원 준비뿐만 아니라 가족 및 가정 환경과 지역사회 및 의료 시스템의 준비가 필요함을 강조하고 있다(Committee on Fetus and Newborn, 2008). 즉, 신생아집중치료실 퇴원 후 가정에서 건강한 성장과 발달을 이룰 수 있도록 점차 고위험신생아 부모의 퇴원 준비가 치료에 중요한 요소로 포함되고 있다(Heo & Oh, 2019; Sannino et al., 2016). 그러나 선행연구에서 많은 부모들이 병원에서 가정으로의 전환에 대해 걱정하고 준비가 되지 않았다고 보고하면서 부모의 ‘퇴원 준비’라는 개념이 등장했다(Ronan et al., 2020).
고위험신생아의 퇴원에 대해 부모는 적절하게 준비되지 않은 경우가 많았으며(Ingram et al., 2016; Smith et al., 2013), 부모의 퇴원 준비가 부족한 경우 신생아의 재입원과 사망의 위험이 증가할 수 있다고 하였다(Kaya et al., 2018). 병원에서 가정으로 퇴원 시 자녀를 돌볼 준비가 되었는지 정확히 판단하는 것은 어려우나, 이를 포괄적으로 측정할 수 있는 도구를 이용하여 고위험신생아의 웰빙과 안전을 추구할 수 있도록 퇴원 전 사정하는 것이 필요할 것이다(Weiss et al., 2015). 세계보건기구(World Health Organization) 지침과 같이 세계적인 권장 사항이 있음에도 불구하고 고위험신생아 부모의 퇴원 준비에 관한 연구는 아직 초기 단계이다(Smith et al., 2022). 국내에서도 고위험신생아 부모의 퇴원 준비에 대한 연구는 드물고, 신생아집중치료실 퇴원을 위한 부모의 퇴원 준비 평가 도구는 거의 없어, 성인을 대상으로 개발된 도구를 부모용으로 수정하여 사용하기도 하였다(Yoon et al., 2019). 또한, 고위험신생아 부모의 퇴원 준비에 대한 체계적인 평가는 아직까지 이루어지지 않은 실정이다(Heo & Oh, 2019). 따라서 고위험신생아 부모를 대상으로 사용되고 있는 퇴원 준비가 어떻게 측정되고 있는지 확인해 볼 필요가 있다. 고위험신생아 부모의 퇴원 준비 정도를 사정 시, 측정도구의 측정속성을 만족시키지 못한 질이 낮은 도구의 사용은 자료의 신뢰성을 위협할 뿐만 아니라 적절한 중재 제공에도 악영향을 미친다. 즉, 신뢰도와 타당도가 검증된 질 높은 측정도구의 사용은 정확한 결과를 얻고 그에 따른 중재 제공에 매우 중요하다(Lee et al., 2013).
측정도구의 질평가와 관련된 다국적 전문가들로 구성된 COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) 위원회는 임상 및 연구에서 사용하는 측정도구를 체계적으로 검토하는 가이드라인을 개발하였다(Mokkink et al., 2010). 점차 COSMIN을 사용한 측정 속성에 대한 체계적 고찰이 급증하고 있으며(Lee et al., 2013), COSMIN 위원회도 측정도구의 다양한 질평가 기준을 문헌 검토 및 전문가 의견을 바탕으로 업데이트를 지속하고 있다(Mokkink et al., 2018; Prinsen et al., 2018). 국내에서도 COSMIN을 사용하여 측정도구의 속성을 분석한 연구들이 점차 진행되고 있으나, 고위험신생아 부모의 퇴원 준비 측정도구를 체계적으로 평가한 연구는 찾아볼 수 없었다.
이에 이 연구는 고위험신생아 부모의 퇴원 준비 측정도구를 파악하고, 문헌에서 사용된 도구의 측정 속성(measurement properties)을 가장 최신의 표준 가이드라인에 따라 체계적으로 평가하고자 한다. 이 연구는 고위험신생아 부모의 퇴원 준비 측정에 대한 문헌고찰을 통해 연구 및 임상에서 적절한 도구 선택에 대한 근거를 마련하고, 측정 도구 개발 및 평가에 대한 연구의 기초자료를 제공하고자 한다.
2. 연구의 목적
이 연구의 목적은 고위험신생아 부모의 퇴원 준비를 측정하는 도구를 확인하고, 측정도구의 측정 속성을 평가하는 것으로, 향후 도구 개발에 필요한 기초자료를 제공하는 데 있다. 구체적인 목적은 다음과 같다.
(1) 고위험신생아 부모의 퇴원 준비를 보고한 연구의 특성(출판연도, 연구 수행 국가, 대상자 집단, 연구 설계 등)과 각 연구에서 사용한 측정 도구(측정도구명, 출판연도, 대상자 및 수, 목적, 개념적 기틀, 영역 및 항목 수, 응답 범주 등)를 파악한다.
(2) 고위험신생아 부모의 퇴원 준비를 측정하기 위해 사용된 도구의 측정 속성의 질(내용타당도, 내적구조, 그 외 측정 속성)을 평가한다.
대상 및 방법
1. 연구 설계
이 연구는 고위험신생아 부모의 퇴원 준비를 측정한 도구의 특성을 고찰하고 측정 속성을 평가하는 체계적 문헌고찰 연구이다. 이 연구에서는 일차적으로 PRISMA (Preferred Reporting Items of Systematic Reviews and Meta-Analysis) 가이드라인에 따라 문헌검색을 진행하여 고위험신생아 부모의 퇴원 준비를 측정하기 위해 사용된 도구를 파악하였다. 이어서 2018 COSMIN 체크리스트(COSMIN risk of bias checklist)를 이용하여 각 도구의 측정 속성을 평가하였다(Mokkink et al., 2018). 문헌의 배제 및 선택부터 측정 속성 분석에 이르기까지 연구의 전 과정은 2명의 연구자가 독립적으로 시행하였다. 검색된 문헌은 체계적 문헌고찰 선정 기준에 따라 독립적으로 검토하였으며, 선정된 문헌을 종합하고 정리하는 과정에서 연구자 간 결과가 일치 여부 확인하고 합의하였다. 2명의 연구자가 선정된 문헌을 독립적으로 검토하고 각 문헌에서 사용된 고위험신생아 부모의 퇴원 준비 측정도구의 특성 및 측정 속성을 평가하였다. 결과의 불일치가 있으면 연구팀의 회의를 통해 합의점을 찾았다. 연구팀은 연구 진행 과정 동안 정기적인 회의를 통해 검색 및 분석을 논의하였다.
2. 핵심 질문
체계적 문헌고찰을 시행하기 위한 핵심 질문은 ‘고위험신생아 부모의 퇴원 준비를 어떻게 평가하는가?’로 선정하였다. 이 연구는 중재에 대한 비교 분석을 위한 연구가 아니므로 문헌고찰을 위한 PICO (Participant, Intervention, Comparison, Out-come) 중 비교중재(C)는 제외하였다. 따라서 이 연구는 PIO를 고위험신생아의 부모(P), 퇴원 준비(I), 사용된 측정도구(O)로 설정하였으며, 질적연구와 리뷰 논문을 제외한 양적 연구 설계(study design)이다.
3. 문헌검색 및 선정
1) 문헌검색
문헌검색은 PIO를 바탕으로 2021년 12월 15일과 16일에 국외 데이터베이스 5개(MEDLINE, Embase, CINAHL, PsycINFO, Web of Science), 국내 3개(대한의학학술지 [KoreaMED], 학술연구정보서비스 [RISS], 한국학술정보 [KISS])를 이용하여 시행하였다. 검색 기간의 제한은 두지 않았으며, 검색 영역은 제목과 초록으로 하였고, 인간 대상 연구로 제한하여 검색하였다.
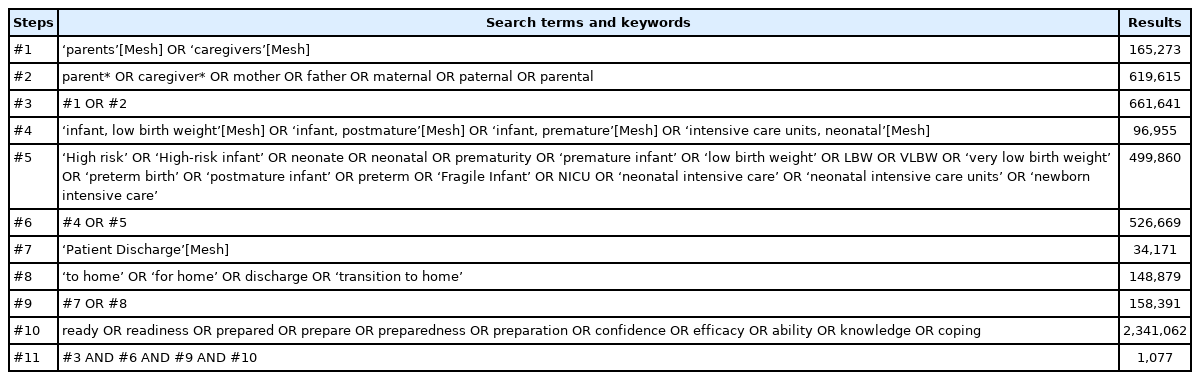
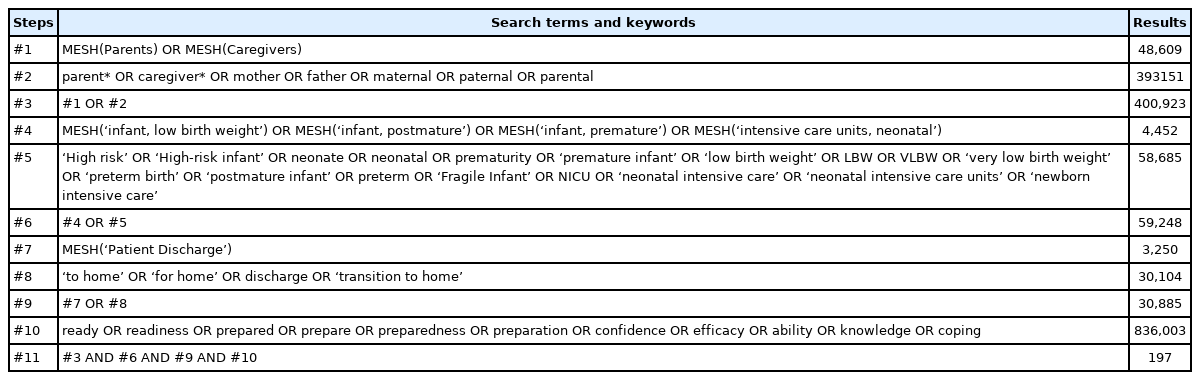
국내 데이터베이스에서는 고위험신생아(premature infant OR low birth weight infant) AND 부모(parents OR caregiver OR family) AND 퇴원(discharge) AND 준비(readiness OR preparation)를 한국어와 영어를 모두 검색어로 사용하여 조합 후 검색하였다. 국외 데이터베이스에서는 관련 의학주제표목(MeSH: medical subject headings), 주요 개념어, 생명과학분야 용어색인(EMTREE)을 AND나 OR과 같은 불리언 논리연산자(Boolean operator)와 절단(truncation)을 조합하여 검색하였다(Appendix 1). 선정된 검색어로 검색하여 총 5,140편(그 중 중복 문헌 2,346편, 논문 취소 1편)의 문헌이 검색되었다(Fig. 1).
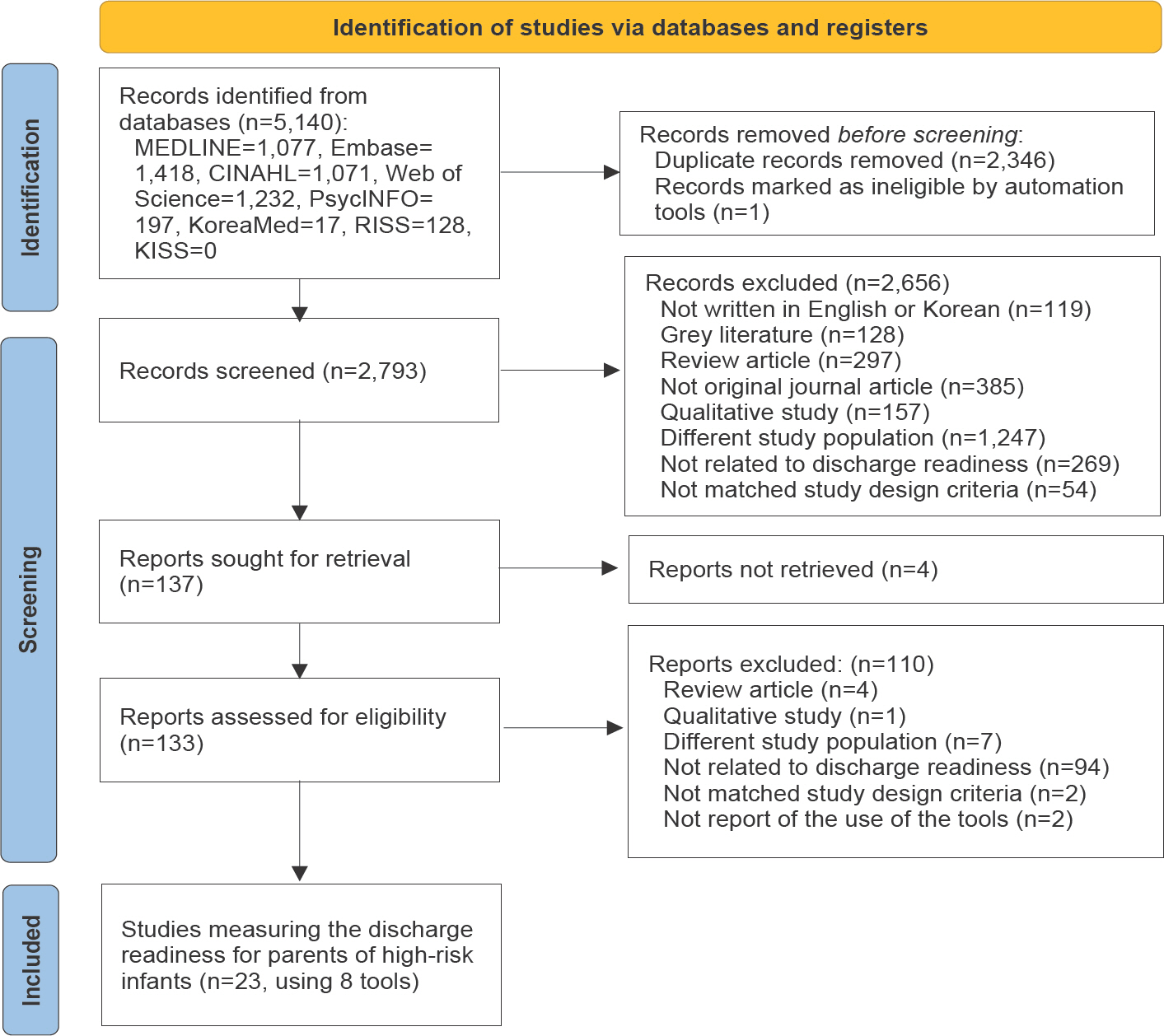
PRISMA (Preferred Reporting Items for Systematic Reviews And Meta-Analyses) flow diagram of the literature search.
2) 문헌 선정
이 연구의 논문 선정 기준은 국내외에서 출판된 논문으로 퇴원 준비를 측정한 도구가 포함되어 있으며, 대상자가 고위험신생아 부모가 포함되어 있으며, 고위험신생아 부모가 응답한 결과를 바탕으로 한 양적연구이다. 고위험신생아 부모의 퇴원 준비를 측정하는 도구의 특성을 조사한 연구와 도구 개발 및 검증 과정과 해당 결과를 보고한 경우도 포함하였다. 배제기준은 영어 또는 한국어 이외의 언어로 출판된 문헌, 학술대회 발표 혹은 초록 게재 논문, 학위논문과 같은 회색 문헌, 고찰(혹은 메타분석) 연구, 질적 연구 논문, 종설(혹은 사설, 프로토콜, 가이드라인 포함), 그리고 전체 원문을 확인할 수 없는 논문이다. 또한, 사용된 측정 도구를 명시하지 않거나 도구의 출처(참고문헌)를 제시하지 않은 논문은 제외하였다. 연구 대상자가 고위험신생아 부모가 아니라, 건강한 신생아, 소아집중치료실(PICU), 소아병동 또는 응급실(혹은 소아응급실) 퇴원 부모를 대상으로 한 경우도 제외하였다. 이러한 기준에 따라 총 23개의 연구에서 사용된 8개의 측정 도구가 최종 확인되었다(Fig. 1).
4. 자료 추출과 분석
검색된 자료는 상용 서지 관리 소프트웨어(EndNote 20.3)를 이용하여 관리하였다. 각 데이터베이스에서 검색된 자료의 중복 자료를 제거한 후 남은 문헌은 논문의 제목과 초록을 확인하여 선택하였다. 이후 선택된 논문은 원문을 검토하여 최종 대상 문헌을 선정하였다. 선정된 논문에서 추출된 자료는 연구자 간 비교할 수 있도록 엑셀 파일을 이용하여 정리하였다.
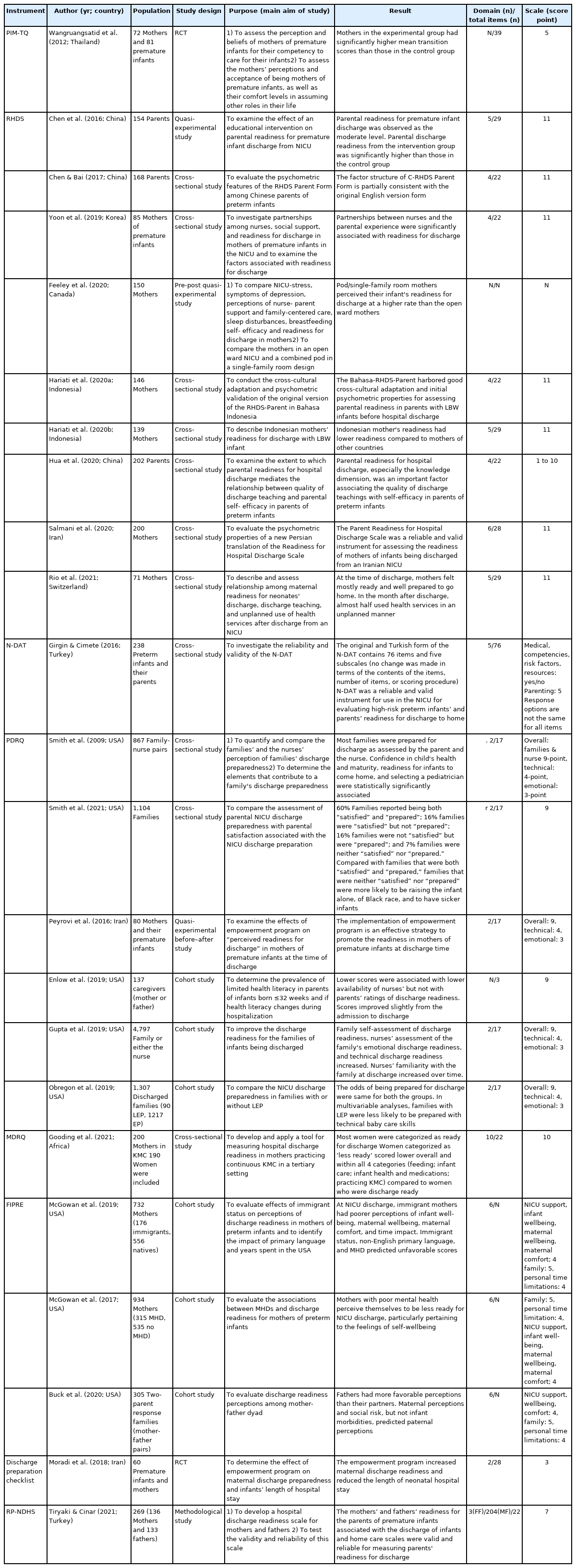
선정된 문헌으로부터 선정 문헌의 특성(저자, 출판연도, 대상자 집단, 연구 설계 등)과 문헌에서 사용한 측정 도구의 특성(측정 방법, 하위 영역, 문항 수, 점수화 방법 등)을 확인하였다(Table 1). 뿐만 아니라, 선정된 문헌에서 사용한 측정도구의 개발과정을 보고한 문헌을 추가적으로 확인하여 측정도구의 특성을 추가 확인하였다(Table 2). 다음으로 선정된 논문에서 사용된 고위험신생아 부모의 퇴원 준비 측정도구의 속성 평가를 하였다(Table 3).
Characteristics of included studies (n=23)

Characteristics of instruments (n=8)

Quality Assessment of the instruments (n=15)
COSMIN은 측정도구의 속성 평가 시 내용타당도, 내적구조, 그리고 그 외 측정 속성의 순서로 평가하도록 하여(Prinsen et al., 2018), 이에 따라 해당하는 자료를 추출, 분석하였다. 측정 도구의 속성에 대한 각 연구는 그 기준에 따라(Appendix 2) 충분(sufficient; ‘+’), 불충분(insufficient; ‘-’), 그리고 불명확(indeterminate; ‘?’)으로 평가하였다(Prinsen et al., 2018). 그 구체적인 정의 및 평가 기준으로, 내용타당도(content validity)는 측정 도구가 측정하고자 하는 개념을 적절히 반영하는 정도로 관련성(relevance)은 측정하고자 하는 개념에 대해 문항이 얼마나 관련 있는지에 대해 평가하는 것이다(Terwee et al., 2018). 내용타당도 지수(content validity index, CVI), 내용타당도 비율(content validity ratio, CVR) 등을 평가한다. 포괄성(com prehensiveness)은 측정 도구에 핵심 개념이 빠지지 않았는지를 평가하고, 이해도(comprehensibility)는 측정도구를 사용하는 대상자들이 적절하게 이해하고 있는지를 평가하였다.
내적구조는 구조타당도(structural validity), 내적일관성(internal consistency), 교차문화타당도/측정동일성(cross-cultural validity/measurement invariance) 등의 보고, 변수에 따른 적절한 지표의 보고를 평가하였다. 구조타당도는 측정하고자 하는 개념의 차원(dimension)을 측정 도구가 적절히 반영하여 측정하고 있는지를 의미하고, 주로 요인분석(factor analysis: confirmatory factor analysis [CFA], exploratory factor analysis [EFA], principal component analysis [PCA])과 문항반응이론(item response theory)이 사용된다. CTT (classical test theory)에서 확인적 요인분석(CFA)를 시행하였다면, comparative fit index (CFI) 또는 Tucker-Lewis Index 가 0.95 초과되었거나 RMSEA (Root Mean Square Error of Approximation)이 0.06 미만이거나 standardized root mean residuals (SRMR)이 0.08 미만이면 충분(sufficient; ‘+’)을 부여하였다. 내적일관성은 문항 간의 상호연관성을 말하며, 주로 Cronbach alpha가 사용되며, 그 값이 0.7 이상이면 충분(sufficient; ‘+’)을 부여하였다. 교차문화타당도/측정동일성은 원 도구의 문항/척도가 번역된 도구의 문항/척도에 얼마나 반영하는지를 의미한다. 다중 집단 요인 분석에서 집단 요인 간에 중요한 차이가 발견되지 않았거나 집단 요인에 대한 중요한 차별기능문항(differential item functioning)이 없으면 충분(sufficient; ‘+’)을 부여하였다.
그 외 측정 속성으로 신뢰도, 측정오차, 준거타당도, 가설검정 구성타당도, 반응도 등의 보고를 평가하였다. 신뢰도(reliability)는 측정이 얼마나 재현될 수 있는지와 같은 측정 도구의 안전성(stability)를 확인하는 것으로, 평가자 간 신뢰도(inter-rater reliability), 검사-재검사(혹은 반복측정 신뢰도; test-retest reliability), 그리고 평가자 내 신뢰도(intrarater reliability)가 있다. 급내상관계수(intraclass correlation coefficient, ICC)나 가중 카파(weighted Kappa)로 확인하며, 0.7 이상이면 충분(sufficient; ‘+’)을 부여하였다. 측정오차는 적을수록 신뢰성이 좋다고 판단하는데(Lee, 2021c), 최저감지변화(smallest detec table change) 또는 일치허용치(limits of agreement)가 최소주요변화(minimal important change)보다 작으면 충분(sufficient; ‘+’)을 부여하였다. 준거타당도(criterion validity)는 측정 도구가 표준화된 측정도구(gold standard)를 얼마나 반영하는지를 의미하며, 동시타당도(concurrent validity)와 예측타당도(predictive validity)가 있다. 표준화된 측정도구와의 상관관계 혹은 area under the curve (AUC)가 0.7 이상이면 충분(sufficient; ‘+’)을 부여하였다. 가설검정 구성타당도(hypo-thesis-testing construct validity)는 연구자가 검정하고자 하는 측정도구와 다른 측정도구로 측정한 결과의 관련성 혹은 차이에 대해 연구자가 미리 가설을 세워, 해당 가설을 만족하였는지를 확인하는 것이다. 이에는 수렴타당도(convergent validity), 판별타당도(discriminant or divergent validity), 그리고 집합타당도(Known-groups validity)가 있다. 결과가 가설에 부합하면 충분(sufficient; ‘+’)을 부여하였다. 반응도(responsiveness)는 시간의 흐름에 따라 측정하고자 하는 개념이 변화하는 것을 감지하는 것을 의미한다. 최소 두 번 이상 측정해야 하며, 측정하고자 하는 개념을 변화시킬 수 있는 중재가 포함되어야 한다. 가설에 따른 결과가 도출되거나 변수에 따른 AUC가 0.7 이상이면 충분(sufficient; ‘+’)을 부여하였다.
결 과
1. 고위험신생아 부모의 퇴원 준비를 보고한 연구의 특성
총 23편의 문헌(국외 문헌 22편, 국내 문헌 1편)이 분석에 포함되었다(Fig. 1, Appendix 1). 2009년과 2012년에 각 1편(4.3 %)을 제외하고 대다수의 문헌(n=21, 91.3%)이 2016년 이후에 출판되었다. 연구가 진행된 국가는 미국 8편(34.8%), 중국 3편(13.0%), 이란 3편(13.0%), 인도네시아 2편(8.7%), 터키 2편(8.7%), 그 외 남아프리카공화국, 스위스, 캐나다, 태국, 한국이 각 1편(4.3%) 순이었다. 대상자 수는 최소 60명에서 최대 4,797명이었으며 고위험신생아 어머니를 대상으로 한 연구가 12편(52.2%), 부모 모두를 대상으로 한 연구가 6편(26.1%), 가족을 대상으로 한 연구가 4편(17.4%), 부모 중 한 명의 양육자를 대상으로 한 연구가 1편(4.3%)이었다. 연구 설계는 횡단조사연구(n=11, 47.8%), 코호트 연구(n=6, 26.1%), 실험연구(n=5, 21.7 %), 방법론적 연구(n=1, 4.3%) 순이었다. 선정된 연구의 특성은 Table 1에 제시하였다.
선정된 23편의 문헌에서 총 8개의 도구가 사용되었으며 도구별 특성은 Table 2에 제시하였다. 선정된 문헌에서 사용된 측정 도구는 Readiness for Hospital Discharge Scale (RHDS) 9편(39.1%), Parent Discharge Readiness questionnaire (PDRQ) 6편(26.1%), Fragile Infant Parent Readiness Evaluation (FIPRE) 3편(13.0%) 순이었고, 나머지 도구는 각 1회씩 사용되었다.
2. 고위험신생아 부모의 퇴원 준비 측정 도구의 특성
각 도구의 특성을 명확하게 고찰하기 위해 각 도구의 개발과정을 보고한 문헌을 추가적으로 고찰하였다. 퇴원 준비 측정 도구 개발 연구를 발표한 국가는 미국이 가장 많았다(n=4, 50%). RHDS는 성인 내과 수술 환자, 산모 및 입원 아동의 부모를 대상으로 개발되었으며, RHDS를 제외한 나머지 7개의 도구는 미숙아 어머니, 부모 혹은 가족을 대상으로 개발되었다. PDRQ는 신생아집중치료실 입원 가족과 간호사의 인식을 비교하기 위하여 가족과 간호사를 쌍으로 측정하도록 개발되었다. FIPRE와 Readiness of Parents with Premature Infants in the Neonatal Intensive Care Unit for Discharge and Home Care Scale (RP-NDHS)는 고위험신생아의 부모를 대상으로 개발되었다. Premature Infant Mothers’ Healthy Transition Questionnaire은 미숙아 어머니를 대상으로 개발되었으며, neonatal discharge assessment tool (N-DAT)는 고위험신생아와 가족을 대상으로 도구가 개발되었다. maternal discharge readiness questionnaire는 캥거루 케어를 시행하는 부모를 대상으로 PDRQ를 수정하여 개발하였다. 측정 도구의 목적은 신생아집중치료실 퇴원 준비에 대한 인식 측정, 위험 요소의 평가, 부모의 정서적 상태, 부모를 포함한 가족의 고위험신생아를 돌보는 지식 및 기술 등을 측정하기 위한 것이었다. 대부분 도구는 선행연구를 기반으로 하는 문헌고찰을 통해 개발되었으며, 그 중에 일부는 문헌고찰과 인터뷰를 포함하여 도구를 개발하였다. 혹은 미국소아과학회 또는 미국산부인과학회의 지침과 같이 증거 기반 프로토콜을 바탕으로 도구를 개발하거나 연구팀의 임상 경험을 추가하여 개발하기도 하였다. 뿐만 아니라 기존에 개발된 도구를 측정 개념에 따르거나 혹은 연구에 맞게 수정하여 개발하기도 하였다.
각 도구의 문항 수는 최소 17개 문항(PDRQ)에서 최대 76개 문항(N-DAT)으로 평균 31.5문항이었다. N-DAT와 PDRQ를 제외한 5개의 도구는 동일한 응답 척도를 이용하였다. N-DAT 는 의료(9문항), 역량(10문항), 위험 요인(24문항), 자원(18문항)은 이분형(Yes/No) 응답으로 채점하며, 문항마다 배점이 다르게 측정되어 있다. 그 중에 양육(15문항)은 5점 Likert 척도(0-4)로 측정한다. PDRQ는 고위험신생아의 가족과 간호사가 쌍으로 설문을 작성하여 점수를 비교하였다. 가족은 신생아집중치료실 퇴원일에 전반적인 퇴원 준비(1문항)에 대해 9점 Likert 척도로 응답한 후 14개의 개별 문항에 대한 답변으로 퇴원 준비를 평가한다. 14문항 중 기술적 전문성 (11문항)은 4점 척도로, 정서적 퇴원 준비(3문항)는 3점 척도 응답하게 하였다. 뿐만 아니라 퇴원 당일 퇴원 간호사가 9점 Likert 척도를 사용하여 가족의 전반적인 정서적(1문항), 기술적(1문항) 퇴원 준비를 독립적으로 평가하였다. 대부분의 측정 도구가 총 점수가 높으면 퇴원 후 전환의 어려움이 적고, 고위험신생아를 돌보는 데 필요한 지식과 기술 측면에서 퇴원의 준비가 된 것을 나타내었으며(Dashti et al., 2014; Gooding et al., 2021; HealthActCHQ Inc., 2010; Smith et al., 2009; Tiryaki & Cinar, 2021; Wangruangsatid et al., 2012; Weiss et al., 2006), 퇴원 준비 관련 위험요인을 평가하는 N- DAT (Robison et al., 2000)는 점수가 낮을수록 퇴원과 관련된 위험이 낮음을 의미하였다.
3. 퇴원 준비 측정 도구 속성의 질 평가
23편의 문헌에서 8편(Enlow et al., 2019; Feeley et al., 2020; Gooding et al., 2021; Gupta et al., 2019; Hua et al., 2020; Obregon et al., 2019; Rio et al., 2021; Smith et al., 2021)은 사용한 도구명(혹은 출처-개발자-)만 명시하고 해당 도구의 신뢰도 및 타당도에 대한 언급이 없어 속성 질평가에서 제외하였다. 그러나 8편을 제외한 나머지 15편의 문헌에서도 COSMIN에서 제시하는 전체 측정 속성 중 포괄성(내용타당도), 교차문화타당도/측정동일성, 측정오차, 준거타당도, 그리고 반응도는 어떤 연구에서도 제시하지 않았다. 퇴원 준비 측정도구 속성의 질 평가에 대한 결과는 Table 3에 제시하였다.
FIPRE를 사용한 3편은 도구 개발에 대한 정보가 없어 내용 타당도 평가를 하지 않았으며, Moradi et al. (2018)는 Dashti 등(2014)의 문헌에서 Discharge preparation checklist의 CVI는 0.99, ICC는 0.88의 내용타당도(관련성)와 신뢰도를 기술하였으나(Moradi et al. 2018), Dashti 등(2014)의 문헌이 페르시아어로 되어 있어 문헌 및 도구를 이해 불가하여 평가하지 않았다. 내용타당도에서 관련성은 5편의 문헌(Girgin & Cimete, 2016; Hariati et al., 2020a; Salmani et al., 2020; Tiryaki & Cinar, 2021; Wangruangsatid et al., 2012)에서 적절한 CVI (or CVR) 수치 혹은 안면타당도의 결과를 명시하고 있었으며, 그 외 2편의 문헌(Hariati et al., 2020b; Peyrovi et al., 2016)은 대상자 또는 전문가(혹은 패널)에게 검정하였다고 기술되어 있으나, 정확한 결과값에 대해서는 제시되어 있지 않았다. 2편의 문헌(Gooding et al., 2021; Smith et al., 2009)은 안면 타당도 검정을 시행하였다고만 기술하였다. 내용타당도에서 이해도는 5편의 문헌(Chen & Bai, 2017; Hariati et al., 2020a; Salmani et al., 2020; Smith et al., 2009; Tiryaki & Cinar, 2021)에서 확인하였다.
측정도구의 내적구조 평가에서 구조타당도는 도구의 속성 질평가를 시행한 전체 문헌 15편 중 40%에 해당하는 6편(Chen & Bai, 2017; Gooding et al., 2021; Hariati et al., 2020a; Salmani et al., 2020; Tiryaki & Cinar, 2021; Wangruangsatid et al., 2012)이 제시하였으며, 그 중 비교 적합 지수(comparative fit index, CFI) 혹은 표준화된 잔차제곱평균제곱근(Standardized Root Mean Residuals; SRMR)의 기준을 만족한 문헌은 2편(Chen & Bai, 2017; Tiryaki & Cinar, 2021)이었다. 도구의 속성 질평가를 시행한 전체 문헌 중 9편의 문헌(60%)에서는 이에 대한 평가를 실시하지 않은 것으로 나타났다(Buck et al., 2020; Chen et al., 2016; Girgin & Cimete, 2016; Hariati et al., 2020b; McGowan et al., 2017; Moradi et al., 2018; Peyrovi et al., 2016; Smith et al., 2009; Yoon et al., 2019). 내적일관성은 도구의 속성 질평가를 시행한 전체 문헌 15편 중 86.7%에 해당하는 13편의 문헌(Buck et al., 2020; Chen & Bai, 2017; Chen et al., 2016; Girgin & Cimete, 2016; Gooding et al., 2021; Hariati et al., 2020a; Hariati et al., 2020b; McGowan et al., 2017; Moradi et al., 2018; Peyrovi et al., 2016; Salmani et al., 2020; Tiryaki & Cinar, 2021; Yoon et al., 2019)에서 도구의 Cronbach alpha를 제시하였다. 그 중 4편의 문헌만이 사용 도구의 각 하위척도의 α값 혹은 범위로 제시하여, 모두 0.7이상임을 확인할 수 있었다(Chen & Bai, 2017; Hariati et al., 2020a; McGowan et al., 2017; Tiryaki & Cinar, 2021). 그 외 2편의 문헌에서는 전체 척도에서는 0.7이상이었으나, 하부척도의 α를 범위로 제시한 값에서 0.7 미만의 값이 제시되어 있었다(Chen et al., 2016; Girgin & Cimete, 2016). 도구의 내적일관성을 Cronbach alpha로 제시한 12편의 문헌 중 나머지 6편(Gooding et al., 2021; Hariati et al., 2020b; Moradi et al., 2018; Peyrovi et al., 2016; Salmani et al., 2020; Yoon et al., 2019)은 전체 척도의 α값만을 제시하고, 하부척도에 대한 α값은 제시되지 않았다. 그 외 한 편의 문헌(Buck et al., 2020)에서는 internal reliability측정을 위하여 Cronbach alphas를 수행하였다고 하였으나, 정확한 수치는 제시되지 않았다.
도구의 속성 질평가를 시행한 15편의 문헌에서 도구의 신뢰도를 제시한 문헌은 총 3편(Girgin & Cimete, 2016; Tiryaki & Cinar, 2021; Wangruangsatid et al., 2012)이었다. 그러나 그 중 한 편(Wangruangsatid et al., 2012)은 도구의 신뢰도가 0.8이라고 기술되어 있으나, 신뢰도가 평가자 간 신뢰도인지, 검사-재검사 또는 반복측정 신뢰도인지, 혹은 평가자 내 신뢰도인지 명시하지 않았다. 평가자 내 신뢰도(intrarater reliability)를 제시한 문헌 한 편(Girgin & Cimete, 2016), 검사-재검사를 mother form과 father form을 각 어머니와 아버지에게 적용하여 ICC값을 제시한 문헌은 한 편(Tiryaki & Cinar, 2021)으로 총 2편의 문헌(13.3%)에서 시행하였다. 문헌들 중에 신뢰도를 평가하였다고 하였으나, 내적일관성(Cronbach alpha)를 제시하거나 혼용하여 사용하는 문헌(Buck et al., 2020; Hariati et al., 2020a; McGowan et al., 2017; Moradi et al., 2018; Peyrovi et al., 2016; Salmani et al., 2020; Tiryaki & Cinar, 2021; Yoon et al., 2019)도 있었다. 구성타당도를 위한 가설검정에서 수렴타당도를 평가한 문헌 한 편(Chen & Bai, 2017), 집합타당도(known-groups validity)를 평가한 문헌 한 편(Girgin & Cimete, 2016)으로 총 두 편의 문헌(13.3%)만이 시행하였다.
고 찰
이 연구는 고위험신생아 부모의 퇴원 준비를 측정한 문헌을 확인하고, 사용된 측정도구의 특성과 측정 속성을 체계적으로 평가하고자 수행하였다. 문헌 검색 및 선정 결과 총 23편이 최종 분석에 포함되었으며, 이들 문헌에서 8개의 도구가 확인되었다. 측정 도구 속성의 질 평가에는 15편의 문헌이 포함되었으며, 이 결과를 중심으로 기술하고자 한다.
선정된 문헌에서 사용된 고위험신생아 부모의 퇴원 준비 측정 도구 8개는 모두 2000년 이후부터 개발되기 시작하였으며, 고위험신생아 부모의 퇴원 준비 관련 연구는 2009년부터 시작되어 2010년 중후반을 기점으로 증가하였고, 다양한 국가에서 연구가 진행되고 있었다. 이는 과거 고위험신생아의 퇴원은 고위험신생아 중심의 퇴원 준비(신체적, 생리적 안정과 같은 건강 상태)가 주된 기준이었으나(Smith et al., 2022), 점차 생존 한계 극복에 따른 퇴원 후 관리의 중요성이 높아지면서 고위험신생아를 돌보는 부모의 퇴원 준비에 대한 관심이 증가하고 있음을 알 수 있다. 국내에서도 고위험신생아 부모의 퇴원 준비에 대한 연구가 보고되었고, 해당 연구에서 국외에서 개발된 측정 도구(RHDS)를 수정·번안한 도구를 사용하였다(Yoon et al., 2019).
선정된 문헌에서 사용된 고위험신생아 부모의 퇴원 준비 측정도구 8개 중 7개는 측정도구의 개발 시 표적 집단은 미숙아를 포함한 고위험신생아의 어머니, 부모 혹은 가족을 대상으로 개발되었다. 그 외 1개 측정도구(RHDS)는 출산모 혹은 병동에 입원한 아동의 부모를 대상으로 표적 집단을 확대하여 가장 널리 사용되고 있었다. 선정된 문헌에서 사용된 고위험신생아 부모의 퇴원 준비 측정도구의 하위영역으로는 고위험신생아 측면(영아의 건강, 상태, 의료적 측면, 웰빙), 신체적 측면(개인 상태, 어머니의 웰빙, 능력: 기술적 전문성, 고위험신생아 간호 능력, 대처 능력, 양육, 수유, 수행), 정서적 측면(미숙아의 어머니가 된다는 것에 대한 수용, 어머니의 편안함, 정서적 퇴원 준비), 정보 및 지식 측면(고위험신생아 돌봄 혹은 간호 관련 지식 및 정보), 자원 측면(기대되는 지원, 가족 결속, 신생아집중치료실 지원)으로 제시하고 있었다.
이 연구에서 선정된 모든 문헌은 포괄성(내용타당도), 교차문화타당도/측정동일성, 측정오차, 준거타당도, 그리고 반응도를 검정하지 않은 것으로 나타났다. 이는 선행연구에서 측정도구 속성 질평가와 비슷한 결과이다(Kim & Lee, 2019; Lee et al., 2020; Lee, 2021a). 2020년에 발표된 측정도구의 속성에 관한 평가 연구에서는 3.7%의 문헌에서만이 내용타당도에서 포괄성을 검토하였다고 보고하였고, 반응도를 보고한 문헌은 없었다고 하였다(Lee et al., 2020). Lee (2021a)도 교차문화타당도/측정동일성에 관한 심리계량적 연구는 찾아보기 힘든 실정이라고 하였으며, Pittsburgh Sleep Quality Index를 중심으로 트라우마 경험자의 수면의 질 측정도구 검토에서도 측정오차를 제시한 연구가 없었다고 하였다(Kim & Lee, 2019). 준거타당도는 측정도구의 표준화된 측정도구(gold standard)를 사용할 수 없는 경우 준거타당도를 평가할 필요가 없으며(Lee et al., 2020), 이미 개발된 도구의 축약형을 개발하는 목적으로 기존 개발된 원 도구(original version)가 사용되는 경우가 아니라면 표준화된 측정도구를 찾기 어렵다(Lee, 2021b). COSMIN 위원회에서도 건강 관련 도구에서 황금표준은 존재하지 않는다고 하여(Mokkink et al., 2018), 준거타당도를 검정한 문헌이 부족하였으리라 생각된다.
타당도는 측정도구가 측정하고자 하는 개념을 실제로 얼마나 측정하는가에 대한 것으로, 내용타당도는 가장 중요한 측정속성으로 간주된다(Prinsen et al., 2018). 그러나 이 연구에서 관련성, 포괄성, 이해력을 모두 포함하여 측정도구의 내용타당도를 평가한 문헌은 없었다. 내용타당도 지수(CVI)를 명확하게 제시한 문헌은 5편(33.3%)이었으나, 대상자와 전문가에게 모두 내용 타당도 결과를 보고한 문헌은 1편(6.7%)이었다. 타당도 지수나 근거를 제시하지 않고 안면 타당도를 확인하였다고만 기술하기도 하였다. 추후 측정도구 개발 혹은 측정도구 속성 평가 시 CVI나 CVR와 같은 객관적인 지표를 이용하여 전문가 집단뿐만 아니라 측정도구를 사용하는 대상자에게도 내용타당도를 평가해야 할 것이다.
구조타당도에서 기준을 만족한 문헌은 2편(13.3%)이었다. 구조타당도를 검증하는 방법으로 요인 분석이 대표적이나(Kim & Lee, 2019), 확인적 요인분석이 탐색적 요인분석보다 실제 수집한 자료와 가설이 얼마나 일치하는지를 확인함에 있어 더 적절한 방법이다(Lee, 2021a). 만약 측정도구의 하부척도에 대한 명확한 근거가 없다면 탐색적 요인 분석을 먼저 시행하고, 모집단과 실제 수집한 대상자 집단에서도 이 결과가 같게 나타나는지를 확인적 요인 분석을 통해 확인하는 교차타당도(cross-validation)을 시행해야 할 것이다. COSMIN 위원회는 내적일관성은 계산 방법의 유사성으로 인해 신뢰도에 포함되지만 개념적 차이를 이유로 별도의 측정 속성으로 간주하기도 하였다(Mokkink et al., 2010). 측정도구의 신뢰도 영역에서 내적일관성에 대한 언급이 없는 문헌 2편(13.3%)을 제외하고, 모두 Cronbach alpha를 이용하여 내적일관성을 보고하였다. 그러나 각 하위척도의 α가 모두 0.7이상인 경우는 4편(26.7%)에 불과하였다. 그 외 내적일관성을 측정하기 위해 Cronbach alpha를 수행하였다고 하였으나 정확한 수치를 제시하지 않았거나(n= 1, 6.7%), 전체 문항에 대한 α만을 제시(6편, 40%)하거나, 각 하위영역의 α를 제시하였으나 0.7 미만 인 경우(n=2, 13.3%)였다. 임상 실무 혹은 연구에서 사용하고자 하는 측정 도구의 내적일관성을 확인하여 충분히 신뢰할만한 지를 확인 후 도구를 적용해야 할 것이다.
측정도구의 신뢰도는 측정도구를 반복 적용 시 일관된 결과가 도출되는지에 대한 것으로, ICC값을 제시한 문헌은 단 2편(13.3%)이었다. 이는 퇴원 준비는 교육, 지지, 경험에 따라 변화하는 특성을 가지므로 검사-재검사 신뢰도를 검정하지 않았으리라 생각한다. 그러나 측정도구의 신뢰도(평가자 간 신뢰도, 검사-재검사 또는 반복측정 신뢰도, 평가자 내 신뢰도 등)가 문헌에서 검정되지 않은 이유에 대한 설명은 없었다. 문헌에 따라서는 측정 도구의 신뢰도를 Cronbach alpha로 제시하고 있어 신뢰도와 내적일관성을 동일한 의미로 나타내고 있기도 하였다. 가설검정 구성타당도를 위하여 수렴타당도 혹은 집합타당도를 제시한 문헌은 단 2편(13.3%)에 불과하였다. 가설검정 구성타당도를 검정하기 위해서는 사용하고자 하는 측정 도구와 비교하고자 하는 측정 도구의 간의 상관관계 정도와 방향에 대한 가설을 세운 후 시행해야 할 것이며, 이는 문헌고찰을 통한 선행연구의 결과를 바탕으로 해야 할 것이다. 이와 같은 방법을 사용한 연구는 10% 내외에 불과하였다. 이는 이 연구에서 선정된 문헌들은 양적연구(실험연구와 조사연구)로서 도구의 신뢰도 및 타당도 검증을 목적으로 하지 않은 문헌이 다량 선정되었으므로 이를 고려할 필요가 있다.
분석에 포함된 8가지의 측정 도구 중 속성의 질 평가에서 모두 충분(sufficient; +)으로 평가된 도구는 없었고, 4개의 속성의 질 평가에서 충분(sufficient; +)로 평가된 도구는 RHDS와 RP-NDHS였다. RHDS는 가장 많이 사용되었으며, 유일하게 국문으로 번역된 도구였다. 고위험신생아 부모의 퇴원 준비를 사정하기 위해 국내에서 개발된 측정도구는 현재 없는 실정이다. 부모의 퇴원 준비에 대한 주제 범위 문헌고찰(scoping review)에서 퇴원 준비 기준을 점차 부모의 신체적 준비, 정서적 준비, 지식과 능력, 자신감, 자원과 환경 등으로 확대할 필요가 있음을 확인하였다(Smith et al., 2022). 이러한 평가 기준의 확대는 고위험신생아 부모의 퇴원 준비에 대한 전체적인 평가를 할 수 있는 측정 도구가 필요하며, 국내의 고위험신생아 부모의 특성, 문화, 자원과 환경에 맞는 도구가 필요함을 의미한다. 고위험신생아의 퇴원 준비를 위해서는 다양한 측면의 검토가 필요하지만, 모든 측면을 동시에 측정하기란 쉽지 않다. 분석에 포함된 도구 중 모든 측면을 고려한 도구는 거의 없었으며, 환경적 영역을 포함한 도구는 없었다. 다양한 측면이 고려된 측정 도구라 하더라도 포함된 많은 문항 수는 측정 도구의 내적일관성을 높이지만, 대상자에게 부담을 주어 피로나 집중력 저하를 초래할 수 있으므로 간명성 측면을 고려해야 할 것이다. 그러므로 고위험신생아의 퇴원 준비에 가장 중요한 핵심 요인이 반영되면서 다차원적인 측면이 고려된 도구의 개발이 필요하다고 볼 수 있다. 각 측정 속성에 맞게 평가된 질 높은 도구의 사용은 올바른 결과 도출과 그에 따른 중재 제공에 중요하지만(Lee et al., 2013), 이 연구의 분석에 포함된 모든 연구에서 측정 도구를 평가하는 속성에 대한 전반적인 정보가 부족함을 확인하였다.
이 연구에서는 한국어와 영어로 출판된 문헌만을 포함하고, 학술대회 발표, 학위논문, 연구 보고서 등 회색 문헌을 배제하였다. 이에 따라 문헌검색 및 선정에서 고위험신생아 부모의 퇴원 준비와 관련된 연구가 모두 포함되지 않았을 가능성이 있다. 또한, 이 연구는 고위험신생아 부모의 퇴원 준비 측정 도구의 현황과 측정 속성을 평가하는 목적으로 시행되어, 고위험신생아 부모의 퇴원 준비 관련 측정 도구들의 장단점을 구체적으로 평가하지 않았다. 그러나 이러한 제한점에도 불구하고 이 연구는 고위험신생아 부모의 퇴원 준비 측정도구를 체계적으로 검토하고, 현재 신생아집중치료실 퇴원을 준비하는 고위험신생아의 부모에게 사용되는 측정도구의 현황과 특성을 확인하였다는 것에 의미가 있다. 또한, 국내의 고위험신생아 퇴원 준비 평가에 대한 현황을 확인하였다. 검토 결과는 고위험신생아 부모의 퇴원 준비를 평가할 수 있는 검증된 도구가 부족하며, COSMIN 의 권고 사항을 활용하는 것과 같이 체계화된 연구 방법을 통해 측정 속성 및 임상적 유용성에 대한 추가 검증이 필요하다는 것을 시사한다. 이 연구는 이러한 결과를 통해 추후 측정도구 개발 및 평가 시 참고할 수 있는 연구 방향 제공 및 국내 대상자에 적합한 도구의 개발 및 평가의 필요성을 제기했다는 것에 의의가 있다.
결 론
이 연구에서는 COSMIN 가이드라인의 평가 기준을 활용하여 고위험신생아 부모의 퇴원 준비 측정 도구의 현황과 측정 속성을 체계적으로 평가하고자 하였다. 최종 23편의 문헌이 선정되었으며, 총 8개의 측정도구가 사용된 것으로 확인하였다. RHDS는 가장 많이 사용된 측정도구이며, 국내 고위험신생아 부모를 대상으로 적용된 유일한 도구이다. 국내에서 개발하여 사용되는 도구는 찾아볼 수 없었다. 이 연구에서 분석한 문헌에서는 측정 도구를 평가하는 속성에 대한 전반적인 정보가 부족함을 확인하였다. 추후 연구에서 국외에서 개발된 측정도구를 국내 임상 및 연구에 사용하기 위해서는 원래 도구의 문항/척도가 번역된 문항/척도에 제대로 반영되는지, 국내 고위험신생아 부모에게 적합한지 먼저 확인해야 할 것이다. 또한, 국내의 사정에 맞는 고위험신생아 부모의 퇴원 준비를 다양한 측면으로 측정하는 도구 개발이 필요하다. 새로운 도구 개발을 할 때 연구자들은 COSMIN 가이드라인과 같은 측정도구의 측정 속성의 질을 평가하는 기준을 참고하여 이를 충족시킬 수 있는 도구를 개발하려는 노력이 필요하다.
Notes
저자는 이 논문과 관련하여 이해관계의 충돌이 없음을 명시합니다.
Acknowledgements
이 논문은 2021년도 연세대학교 간호대학 김모임연구소 교수-학생 연구비 지원에 의하여 이루어진 것임.